
Introduction
The shoulder joint is a ball and a shallow socket joint. Above the ball and socket joint is a ligament which is attached to a bony prominence (acromion) on your shoulder blade. This forms an arch. The area between the shoulder joint and the arch is known as the sub-acromial space. To move your shoulder and control the position of the ball on the socket, you have a group of muscles and tendons known as the rotator cuff. They attach from the shoulder blade onto the top of the arm bone, passing through the sub-acromial space. One tendon (‘supraspinatus’) sits in the middle of the sub-acromial space. A small fluid lining (‘bursa’) cushions the tendon from the roof of the arch. When you move your arm away from your side, the rotator cuff works to keep the ball centred on the socket. When your arm reaches shoulder height(horizontal), the sub-acromial space is narrowed. Above and below the horizontal, the space is larger.

What is impingement?
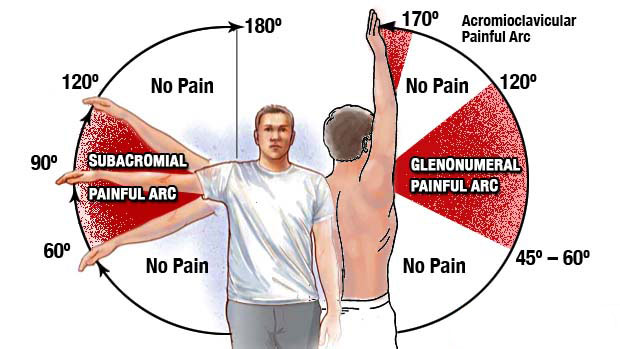
When we raise our arm to shoulder height, the space between the acromion and rotator cuff narrows. The acromion can rub against (or “impinge” on) the tendon and the bursa, causing irritation and pain.
Cause
Rotator cuff pain is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball, and tennis are particularly vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as paper hanging, construction, or painting are also susceptible. Pain may also develop as the result of a minor injury, poor posture Sometimes, it occurs with no apparent cause.
Some people are predisposed to impingement because of hooked or down sloping acromion.
Symptoms
You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position.
Earlier symptoms may be mild, symptoms may include:
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
Examination
Firstly, other causes which mimics shoulder pain will be ruled out like pinched nerve, secondary to cervical spondylosis, also ac joint arthritis and glenohumeral arthritis to be ruled out.
Diagnostic tests
X-rays to rule out arthritis
MRI and ultrasound scan to confirm the problem, sometimes partial tear of rotator cuff is seen.
Treatment
Treatment is usually non-surgical, with a very small proportion of people requiring an operation. An operation is usually only done when your shoulder has not responded to the following ‘conservative’ (non-surgical) treatments.
The majority of people find their symptoms settle without the need for an operation
NSAID’S, cortisone injections, pain reliever gels
Physiotherapy An assessment of your shoulder will be done, and from this, an individual programme of exercises given. These may include exercises to strengthen the muscles around your shoulder blade, improve your posture, stretching exercises and/or strengthening the rotator cuff. Although the exercises may be hard work, tight or uncomfortable, they should not be painful. If you are unable to do any form of exercise because of pain, the physiotherapist may offer treatments such as ultrasound and laser.
Surgical treatment
If your symptoms do not settle with the above measures, an operation may be suggested. The operation done most frequently is a ‘sub-acromial decompression’ (SAD). This is done by keyhole surgery (arthroscopy) and you are in hospital for a day. The operation involves cutting the ligament and shaving away part of the prominence on the underneath of the acromion bone. This aims to increase the size of the sub-acromial space. If the rotator cuff muscle is torn, the surgeon will repair it. Rehabilitation after the repair operation is longer than after the decompression operation alone.
Follow us